What The Most Rigorous Assessment Available Found
Apr 20, 2026
In 2019, a family court judge concluded that Kate Markland was emotionally unfit to parent.
No formal psychological assessment by a qualified psychologist or psychiatrist was conducted. No clinical tools validated for the assessment of parenting capacity were applied. No GP records were requested or reviewed.
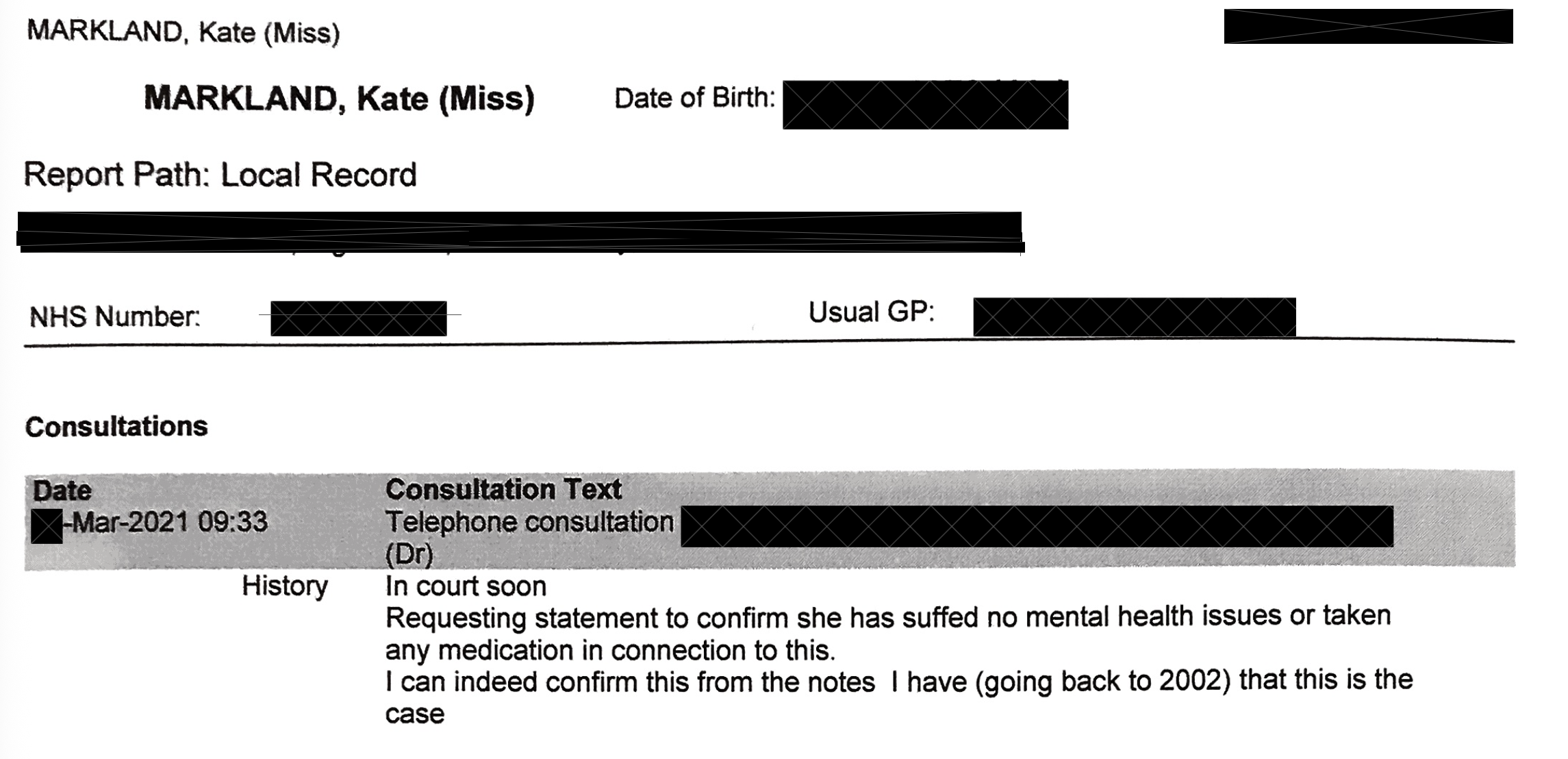
The GP records, which Kate is making available, show nothing. No entries consistent with significant mental health difficulties. No referrals to mental health services. No medication for psychiatric conditions. No clinical history that would support a finding of emotional unfitness.
The question this raises is precise: what was the 2019 assessment actually measuring?
What a valid psychological assessment requires
The British Psychological Society and Family Justice Council publish joint statutory guidance, Psychologists as Expert Witnesses in the Family Courts in England and Wales (January 2016), setting out the minimum standards for any psychological assessment instructed by the court. The guidance is explicit: a valid assessment requires validated tools, a qualified and regulated practitioner registered with the HCPC or chartered by the BPS, access to relevant records including medical history, and sufficient time to distinguish enduring patterns from situational responses. An assessment that does not meet these standards is not a valid psychological assessment. It is, in the BPS's own framing, an assessment that is incomplete and whose conclusions cannot be relied upon.
Those tools are designed to separate what a person is like from how a person presents under adversarial pressure. That distinction is not a technicality. It is the entire basis on which a clinical finding can be distinguished from an impression.
Daniel Siegel's work on the developing mind (Siegel, 2020, 3rd ed.) documents how the brain responds to threat. The stress response system produces precisely the behaviours that, viewed out of context, might be misread as evidence of emotional instability: difficulty regulating emotion, difficulty presenting a calm and coherent narrative, physiological signs of distress. These are not symptoms of disorder. They are the normal neurological response to threat.
Assessing someone's emotional fitness in an adversarial legal environment and concluding that the distress they display is evidence of unfitness is not a clinical finding. It is a circular argument.
The Cambridge finding
In 2019, the same year as the assessment, University of Cambridge researchers published findings that family court decisions are routinely distorted by the misuse of key psychological research. The researchers specifically identified the misapplication of attachment theory and parental alienation frameworks as producing decisions that were not clinically valid.
They were not commenting on any individual case. They were commenting on a systemic pattern. That pattern is directly relevant to the validity of any assessment that relied on contested frameworks rather than validated clinical tools.
What the GP records show
Kate's GP records span nearly two decades. They show no history of mental health concerns. No referrals to specialist services. No prescription of psychotropic medication. No documented psychiatric concerns of any kind.
In evidence-based clinical practice, a longitudinal absence of clinical history is not irrelevant. It is part of the assessment. It is, in fact, core clinical evidence.
A finding of emotional unfitness made without reference to the GP record is not a complete assessment. It is an incomplete one that reached a conclusion the available evidence did not support.
What the subsequent assessment showed
A comprehensive psychological assessment was later conducted using established, validated instruments: the Millon Clinical Multiaxial Inventory–III (MCMI-III), the Beck Depression Inventory–II (BDI-II), and the Beck Anxiety Inventory (BAI). These are widely used clinical tools with strong reliability and validity in both clinical and forensic settings, designed to assess enduring personality patterns as well as current psychological difficulties.
The results were unambiguous. The response profile was assessed as valid and reliable. Across all measures, there was a clear absence of psychological difficulty.
No evidence of depression. No evidence of anxiety. No indication of personality disorder or emotional instability.
The clinical conclusion was straightforward: there are no psychological, personality, or emotional issues that would prevent Kate from providing good enough parenting.
Beyond mental health, the full clinical picture is consistent across every line of evidence. No history of substance misuse. No alcohol dependency. No offending history. GP records spanning nearly two decades with no mental health concerns. These are the factors routinely examined in parenting assessments because of their known association with impaired parenting capacity. Their absence, across two decades of documented history, is clinically significant.
Kate voluntarily subjected herself to the most rigorous clinical assessment available
It is worth being precise about what happened here. Kate was not assessed by the court using validated tools. Kate was not asked to engage with a qualified clinical psychologist using standardised instruments. The 2019 determination was made without any of that.
Kate arranged it herself.
Of her own volition, and at her own initiative, Kate sought out and submitted to a comprehensive psychological assessment using the MCMI-III, the BDI-II, and the BAI — the validated clinical instruments the court process never applied. She did not do this under compulsion. She did not do this because a court ordered it. She did this because she was confident the evidence would speak for itself, and because she understood that the standard the court had applied was not a clinical standard at all.
The results confirmed what two decades of GP records already showed. No depression. No anxiety. No personality disorder. No barriers to parenting. A valid and reliable response profile across every measure.
A person who is concealing psychological instability does not voluntarily seek out the most rigorous clinical assessment available and make the results public. A person who knows the evidence is on their side does.
The contrast between what Kate chose to do and what the 2019 process failed to do is not incidental. It is the point.
The contrast
The 2019 finding was reached without validated tools, without a qualified and regulated practitioner conducting the assessment, and without access to the GP records that form a core part of any valid clinical picture.
The BPS and FJC guidance is unambiguous: without these elements, a conclusion about emotional fitness to parent is not a valid psychological assessment. It is an observation made in an adversarial environment, elevated to a clinical finding without the methodology to support it.
The subsequent assessment meets every standard the 2019 process did not. Validated instruments. Corroborating medical history spanning two decades. Consideration of established risk factors. A qualified practitioner. A response profile assessed as valid and reliable.
Its conclusion is supported across every available line of evidence. The 2019 conclusion is not.
A finding of emotional unfitness that does not use validated tools, does not review the available clinical record, and is not conducted by a qualified and regulated practitioner is not a clinically grounded finding. It is an inference drawn from an incomplete process.
The issue is not interpretation. It is professional overreach.
The BPS and FJC guidance is explicit about who is qualified to assess parenting capacity in a family court context: a practitioner psychologist registered with the HCPC or chartered by the BPS, using validated instruments, with access to the full clinical record. The guidance exists precisely because these assessments carry life-changing consequences and cannot be left to unqualified observation.
The 2019 determination was not made by a qualified and regulated psychologist using validated tools. It was made by a legal process that assessed presentation in an adversarial environment and elevated that observation to a clinical conclusion.
That is not an assessment. It is a finding dressed as one.
The subsequent clinical evidence, validated instruments, two decades of GP records, no mental health history, no substance misuse, no offending history, clear results across every measure, does not merely tell a different story. It exposes the 2019 conclusion for what it was: a determination made outside the competence of those who made it, using a process the governing bodies of clinical psychology explicitly say is insufficient.
Kate did not fail a clinical assessment. No valid clinical assessment was conducted. What was conducted fell outside the regulatory and methodological standards that exist to protect people from exactly this outcome.
The harm to Kate and Gabriel was not the result of a fair process that reached the wrong conclusion. It was the result of professionals operating beyond the boundaries of their qualification and competence, in a system that permitted them to do so without clinical accountability.
That is professional overreach. And the evidence, sourced entirely from the profession's own governing bodies, says so.
References
- British Psychological Society and Family Justice Council. (2016). Psychologists as Expert Witnesses in the Family Courts in England and Wales: Standards, Competencies and Expectations. Joint guidance from the Family Justice Council and the British Psychological Society. Leicester: British Psychological Society. Available at: www.bps.org.uk
- Siegel, D. J. (2020). The developing mind: How relationships and the brain interact to shape who we are (3rd ed.). New York: Guilford Press. ISBN: 9781462542758.
- Duschinsky, R., Forslund, T., Granqvist, P. et al. (2021). Attachment goes to court: Child protection and custody issues. Attachment & Human Development. DOI: 10.1080/14616734.2020.1840762 [University of Cambridge-led international consensus statement identifying systemic misuse of attachment research in family court decisions.]
- Millon, T. (1994). Millon Clinical Multiaxial Inventory–III manual. Minneapolis: National Computer Systems. [MCMI-III: validated clinical instrument used in the subsequent assessment.]
- Beck, A. T., Steer, R. A. & Brown, G. K. (1996). Beck Depression Inventory–II. San Antonio: Psychological Corporation. [BDI-II: validated clinical instrument used in the subsequent assessment.]
- Beck, A. T. & Steer, R. A. (1990). Beck Anxiety Inventory manual. San Antonio: Psychological Corporation. [BAI: validated clinical instrument used in the subsequent assessment.]






